
Albinism vs Vitiligo: 7 Shocking Differences
Introduction: Beyond the Pale
In a world where human diversity is most visibly expressed through skin, hair, and eye color, conditions that alter pigmentation often generate curiosity and, unfortunately, misunderstanding. At first glance, terms like albinism and vitiligo are often used interchangeably in public discourse; however, they represent fundamentally distinct conditions with separate origins, mechanisms, and implications. Therefore, this comprehensive analysis moves beyond superficial observation to uncover and explain the intricate biological narratives of albinism vs vitiligo.
Furthermore, we will place them in a broader context by comparing them to other pigmentary disorders like leucism, piebaldism, and melanism etc. We will dissect their genetic blueprints, pathological processes, and clinical presentations, providing clarity for healthcare professionals, researchers, and the intrigued public alike.
The Fundamental Divide: Congenital Absence vs. Acquired Loss
The most critical distinction in the albinism vs vitiligo discussion lies in their very nature. One (albinism) is a lifelong genetic inheritance, while the other is typically an acquired autoimmune (vitiligo) phenomenon.
Albinism – A Genetic Script from Birth
Albinism is not a single disorder but a group of inherited genetic conditions. Consequently, individuals are born with it, and the condition persists for life. The core defect involves a mutation in one of several genes responsible for the production of melanin. Melanin is the primary pigment that gives color to our skin, hair, and eyes. These genetic errors result in a significantly reduced or completely absent melanin synthesis from the moment of birth. Importantly, this genetic blueprint affects the entire body systemically, meaning all skin surfaces and the eyes (ocular albinism) are involved.
Vitiligo – The Body Turning on Itself
In stark contrast, vitiligo is an acquired condition. It most commonly manifests later in life—often during the teens, twenties, or thirties—although it can occur at any age. Most importantly, vitiligo is widely classified as an autoimmune disorder. In fact, for reasons not yet fully understood, the body’s own immune system mistakenly identifies and attacks melanocytes—the specialized cells responsible for producing melanin. Consequently, this immune misrecognition becomes the central mechanism behind the progressive pigment loss characteristic of the condition. As a result, this targeted destruction leads to a progressive loss of pigment in well-defined patches of skin. Thus, while albinism represents a story of faulty production, vitiligo unfolds as a narrative of targeted destruction.
Under the Microscope: Dissecting the Pathophysiological Pathways
Understanding the albinism vs vitiligo dichotomy requires a deeper look into the cellular and molecular mechanisms at play.
The Melanin Synthesis Pathway Breakdown in Albinism
Research has identified several genes whose mutations can cause various types of albinism (e.g., OCA1, OCA2, OCA3, OCA4). The most common types involve mutations in genes encoding the enzyme tyrosinase (TYR) or proteins that help structure the melanosome (the organelle where melanin is made). For instance:
- OCA1 (Tyrosinase-related Albinism): Mutations in the TYR gene lead to a non-functional or absent tyrosinase enzyme. This enzyme is the critical catalyst for the first step of melanin production. Without it, the entire synthesis pathway grinds to a halt.
- OCA2 (The Most Common Type): Mutations affect the OCA2 gene, which codes for a protein crucial for the proper pH and structure of the melanosome. This creates a hostile environment for melanin production, drastically reducing output.
The result is a congenital, systemic lack of melanin. This deficit has profound implications, which we will explore in the clinical presentation section.
The Autoimmune Attack in Vitiligo
The pathophysiology of vitiligo is a complex cascade of autoimmune activity. Key research findings point to a multi-step process:
- Initial Trigger: Genetic predisposition, combined with environmental factors like stress, skin trauma (Koebner phenomenon), or sunburn, may initiate the process.
- Immune Activation: Cytotoxic CD8+ T cells become activated and specifically target melanocyte antigens, such as tyrosinase.
- Cellular Destruction: These T cells infiltrate the skin and release inflammatory signals (e.g., IFN-γ) which further recruit other immune cells. They directly initiate apoptosis (programmed cell death) in melanocytes.
- Loss of Pigment: The destroyed melanocytes can no longer produce melanin, leading to the characteristic white macules and patches.
Ongoing research is intensely focused on elucidating the precise triggers and the role of the innate immune system to develop more targeted therapies.
A Clinical Comparison: Manifestations and Management
The stark differences in origin and mechanism between albinism vs vitiligo translate directly into their visible and systemic presentations (Table 1).
| Table 1: Comparison of Albinism and Vitiligo | ||
| Feature | Albinism | Vitiligo |
| Onset | Congenital (present at birth) | Acquired (usually appears later in life) |
| Pattern | Systemic & Symmetrical: Uniformly light skin, hair, and eyes across the entire body. | Focal & Often Symmetrical: Well-demarcated, milky-white patches that can spread unpredictably. |
| Hair | Hair is white, off-white, or very light blonde from birth. | Patches of white hair (poliosis) can appear only in areas where vitiligo affects the skin. |
| Eye Involvement | Always present. Includes nystagmus (involuntary eye movements), photophobia (light sensitivity), reduced visual acuity, and misrouting of optic nerves. | Eyes are typically not affected in terms of vision. The retina is usually unharmed, though some may have minor pigment changes in the iris. |
| Sun Sensitivity | Extremely high risk of severe sunburn and skin cancer due to complete lack of protective melanin. | Affected patches have no protection and burn easily. Normally pigmented skin has standard protection. |
Management Strategies: Protection vs. Repigmentation
The management goals for these two conditions differ significantly:
- For Albinism: Management of albinism is primarily preventive and protective. Above all, the cornerstone is rigorous, lifelong sun protection—this includes high-SPF broad-spectrum sunscreen, protective clothing, and UV-filtering sunglasses. In addition, regular dermatological screenings are essential for early detection of skin cancer, while consistent ophthalmological care helps address vision problems. Since there is currently no cure, treatment focuses on minimizing health risks, preserving vision, and ultimately maximizing quality of life for affected individuals..
- For Vitiligo: Management aims to stop progression and encourage repigmentation. Treatments include:
- Topical Corticosteroids/Calcineurin Inhibitors: To suppress local immune activity.
- Phototherapy (Narrowband UVB): The gold standard treatment to stimulate melanocyte migration and repigmentation.
- JAK Inhibitors: A groundbreaking new class of drugs (e.g., ruxolitinib cream) that target specific immune pathways, showing significant repigmentation success.
- Depigmentation Therapy: For extensive vitiligo, chemically removing pigment from remaining normal skin to create a uniform appearance.
- Surgical Techniques: Melanocyte transplantation for stable vitiligo.
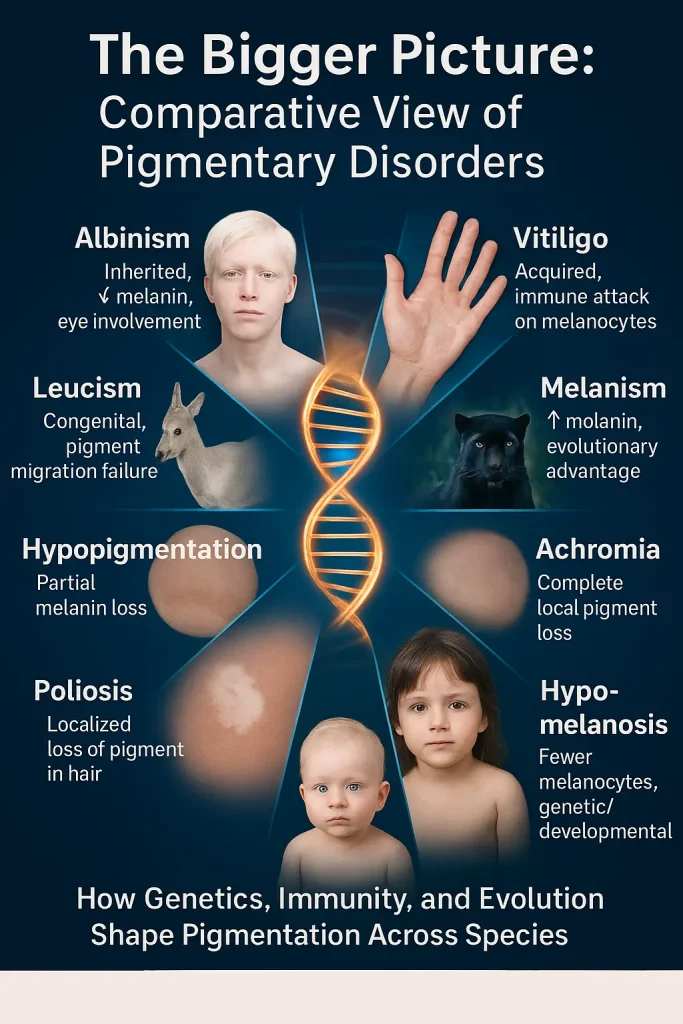
The Bigger Picture: A Comparative Table of Pigmentary Disorders
To fully understand albinism vs vitiligo, we must contextualize them within the wider spectrum of pigmentary conditions. The following table provides a clear, research-oriented comparison (Table 2) and infographic image.
Classification and Comparison of Pigmentary Disorders
| Table 2: Classification and Comparison of Pigmentary Disorders | ||||
| Term | Category | Primary Cause/Mechanism | Key Characteristics | Species Prevalence |
| Albinism | Genetic Disorder | Mutation in genes crucial for melanin synthesis (e.g., TYR, OCA2). | Congenital, systemic reduction or absence of melanin in skin, hair, and eyes. Associated with vision problems. | Humans & Animals |
| Vitiligo | Autoimmune Disorder | Immune-mediated destruction of melanocytes. | Acquired, progressive, well-defined white patches on the skin. May have poliosis (white hair). | Primarily Humans |
| Leucism | Genetic Disorder | Partial defect in melanoblast migration, development, or differentiation during embryogenesis. | Congenital, partial loss of pigment in the skin/hair, but eyes have normal pigmentation. Crucial distinction from albinism. | Primarily Animals |
| Melanism | Genetic Adaptation | Overproduction of melanin, often due to mutation in the MC1R gene or other regulators. | Darkening of skin, hair, or fur. Often an evolutionary adaptation for camouflage (e.g., black panthers). | Humans & Animals |
| Hypopigmentation | Descriptive Term | Umbrella term for any condition characterized by reduced melanin production. | Describes the state of having less pigment. Vitiligo, albinism, and piebaldism are all forms of hypopigmentation. | Humans & Animals |
| Achromia / Achromasia | Descriptive Term | Complete absence of melanin. | A more severe form of hypopigmentation. The patches in vitiligo are achromic. Albinism is a form of total achromia. | Humans & Animals |
| Poliosis | Clinical Sign | Localized absence of melanin in hair follicles. | A circumscribed patch of white or gray hair. It is not a condition itself but a symptom seen in vitiligo, piebaldism, and other disorders. | Humans & Animals |
| Piebaldism | Genetic Disorder | Mutation in the KIT proto-oncogene, affecting melanoblast migration. | Congenital, stable white patch (often with poliosis) typically on the forehead and ventral body. A forme fruste of leucism in humans. | Humans & Animals |
| Hypomelanosis | Pathological Term | Umbrella term for disorders with a reduced number of melanocytes or reduced melanin synthesis. | Often used interchangeably with hypopigmentation in medical literature to describe the pathological process. | Humans & Animals |
Societal Perception and Psychological Impact
Finally, the journey of albinism vs vitiligo intersects profoundly with psychosocial well-being. Both conditions can subject individuals to stigma, staring, and bullying due to their visible difference.
- Albinism: In many parts of the world, particularly in sub-Saharan Africa, individuals with albinism face extreme discrimination, violence, and harmful myths. Globally, navigating a world not designed for extreme light sensitivity and visual impairment presents daily challenges.
- Vitiligo: The unpredictable and often progressive nature of vitiligo can cause significant psychological distress, anxiety, and loss of self-esteem. The visible patches can lead to unwanted questions and social anxiety.
Therefore, comprehensive care for both conditions must include psychological support, public education, and community advocacy to combat stigma and promote inclusivity.
Note: For further reading, see our related article on human diseases and the genetic factors that influence them, such as Sickle Cell Disease, Autism, Cystic Fibrosis, Huntington’s Disease and other inherited disorders.
Conclusion: albinism vs vitiligo: Two Stories, One Goal for Understanding
The narrative of albinism vs vitiligo is a powerful testament to the complexity of human biology. On the one hand, albinism represents a genetically programmed absence of pigment production; on the other hand, vitiligo reflects an immune-mediated destruction of pigment-producing cells. In essence, one is systemic and stable from birth, whereas the other is focal, acquired, and potentially progressive.
Consequently, among researchers, this distinction drives entirely separate investigative pathways: one in genetic therapy and the other in immunomodulation. Similarly, clinicians recognize that it dictates divergent diagnostic and treatment algorithms. For the public, understanding this difference—along with the broader vocabulary of pigmentary disorders—is the first step toward replacing misconception with empathy and support. Ultimately, by appreciating the profound scientific distinctions between these conditions, we can better support the individuals who live with them and, in turn, contribute to a more informed and compassionate world.
References & Further Reading
Key Organizations for albinism and vitiligo Patients & Clinicians:
- National Organization for Albinism and Hypopigmentation. (n.d.). Home. Retrieved May 16, 2024, from https://www.albinism.org/
- Vitiligo research foundation. (n.d.). Retrieved September 8, 2025, from https://vrfoundation.org/
Core Review Articles (Foundational Support):
- Gronskov, K., Ek, J., & Brondum-Nielsen, K. (2007). Oculocutaneous albinism. Orphanet Journal of Rare Diseases, 2(1), 43. https://doi.org/10.1186/1750-1172-2-43
- Rodrigues, M., Ezzedine, K., Hamzavi, I., Pandya, A. G., & Harris, J. E. (2017). New discoveries in the pathogenesis and classification of vitiligo. Journal of the American Academy of Dermatology, 76(1), 1–13. https://doi.org/10.1016/j.jaad.2016.10.048
- Oiso, N., Fukai, K., Kawada, A., & Suzuki, T. (n.d.). Piebaldism. The Journal of Dermatology, 40(5), 330–335. https://doi.org/10.1111/j.1346-8138.2012.01583.x
Latest Research & Breakthroughs (For Further Reading):
On Vitiligo Pathogenesis & Treatment:
- Liu, K., Zhou, L., Shi, M., Cong, T., Yang, X., Zhou, X., Cheng, M., Ma, C., Yao, S., Ying, P., Mu, Z., & Wu, Y. (2024). JAK inhibitors in immune regulation and treatment of vitiligo. Cytokine & Growth Factor Reviews, 80, 87–96. https://doi.org/10.1016/j.cytogfr.2024.11.002
- Harris, J. E., Pandya, A. G., Lebwohl, M., Grimes, P., Gottlieb, Ab., Sofen, H. L., Moore, A. Y., Butler, K., Sun, K., & Rosmarin, D. (2021). 312 safety and efficacy of ruxolitinib cream for the treatment of vitiligo: 104-Week data from a phase 2 study. Journal of Investigative Dermatology, 141(10), S202.
- https://doi.org/10.1016/j.jid.2021.08.319
On Albinism & Novel Therapies:
- Liu, S., Kuht, H. J., Moon, E. H., Maconachie, G. D. E., & Thomas, M. G. (2021). Current and emerging treatments for albinism. Survey of Ophthalmology, 66(2), 362–377. https://doi.org/10.1016/j.survophthal.2020.10.007
- Adams, D. R., Menezes, S., Jauregui, R., Valivullah, Z. M., Power, B., Abraham, M., Jeffrey, B. G., Garced, A., Alur, R. P., Cunningham, D., Wiggs, E., Merideth, M. A., Chiang, P. W., Bernstein, S., Ito, S., Wakamatsu, K., Jack, R. M., Introne, W. J., Gahl, W. A., & Brooks, B. P. (2019). One-year pilot study on the effects of nitisinone on melanin in patients with OCA-1B. JCI insight, 4(2), e124387. https://doi.org/10.1172/jci.insight.124387
On Psychosocial Impact:
- Linthorst Homan, M. W., Spuls, P. I., de Korte, J., Bos, J. D., Sprangers, M. A., & van der Veen, J. P. (2009). The burden of vitiligo: patient characteristics associated with quality of life. Journal of the American Academy of Dermatology, 61(3), 411–420. https://doi.org/10.1016/j.jaad.2009.03.022
Frequently Asked Questions about Albinism and Vitiligo
Is albinism a disability?
Albinism itself is not classified as a disability, but it can lead to certain impairments. Many people with albinism have vision problems such as nystagmus, photophobia, or reduced visual acuity, which may qualify as a disability in some contexts. Social stigma and lack of awareness can also create challenges. However, with proper eye care, sun protection, and supportive environments, most individuals with albinism can lead healthy and productive lives.
How to prevent albinism during pregnancy?
Currently, there is no way to prevent albinism, as it is a genetic condition inherited when both parents pass on the altered gene. However, couples with a family history of albinism can undergo genetic counseling before pregnancy to assess risks. Prenatal testing methods, such as chorionic villus sampling (CVS) or amniocentesis, can help identify whether the fetus has inherited the condition.
Which is the basic unit of heredity that carries the trait of albinism from parent to offspring?
The basic unit of heredity is the gene. Albinism occurs due to mutations in genes responsible for melanin production, such as the TYR gene. When both parents carry and pass on a mutated gene, their child may be born with albinism.
Did Michael Jackson have vitiligo?
Yes, Michael Jackson publicly revealed that he had vitiligo, a condition that causes loss of skin pigmentation. Vitiligo is different from albinism, as it is not inherited at birth but develops when the body’s immune system attacks pigment-producing cells.
What is the difference between albinism and vitiligo?
Albinism is a genetic condition present from birth, affecting skin, hair, and eye pigmentation. Vitiligo, on the other hand, is an acquired autoimmune condition that develops later in life and causes patchy loss of skin color.
Can people with albinism live a normal life?
Yes. With sun protection, proper eye care, and regular medical support, people with albinism can live long, fulfilling lives, pursue education, and build careers. Awareness and inclusion are key to reducing social barriers.





