AI Genetic Diagnosis: Can a Machine Really Spot the One Faulty Gene?
MEDICAL DISCLAIMER
This article is for educational purposes only. No AI system discussed here has regulatory authorization for autonomous genetic diagnosis without human oversight. All clinical decisions should be made with qualified healthcare professionals.
Introduction: Think of It Like a High-Tech Metal Detector
Imagine you are searching for a lost earring on a vast beach. Millions of grains of sand. You cannot examine every one. So you bring a metal detector.
It beeps only where metal is present. It narrows your search from millions to a handful of spots. Then you dig. You find the earring.
That is exactly what AI does in genetic diagnosis.
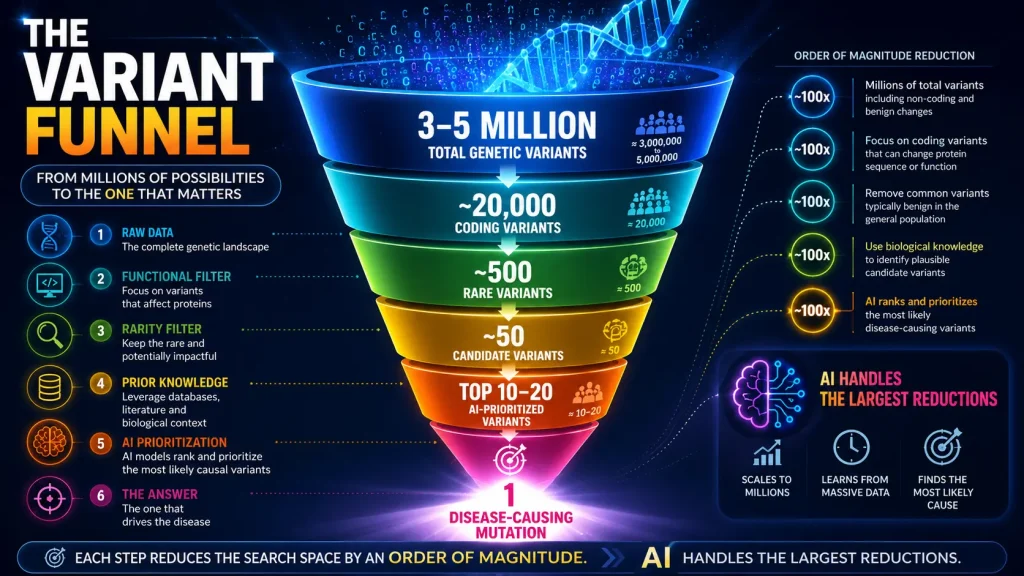
A human genome contains over 3 billion DNA letters. Sequencing reveals between 3 and 5 million differences from a reference genome. Most are harmless. Somewhere among them — often just one or two — lies the disease-causing mutation.
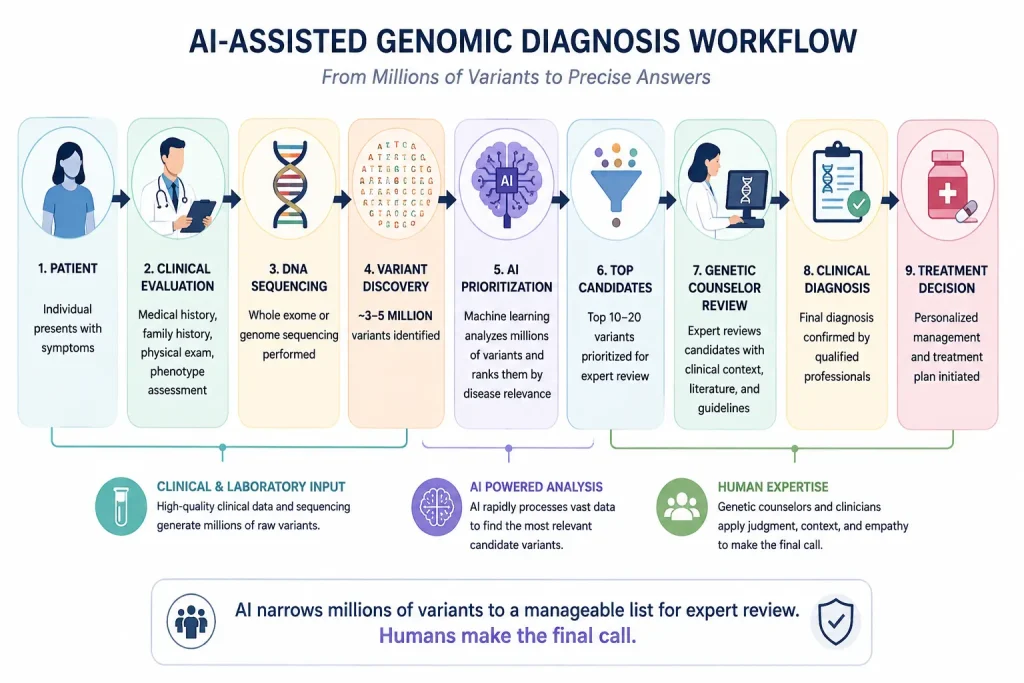
AI acts as the metal detector. It scans millions of variants and flags the most promising candidates. Then a genetic counselor or clinical geneticist reviews those candidates and makes the final diagnosis.
Can a computer really find a disease-causing mutation?
Yes. In research settings, it can.
A recent AI tool called V2P ranked the correct genetic variant in the top 10 candidates over 85% of the time in retrospective evaluations (Stein et al., 2025).
But here is the crucial distinction. That number comes from a benchmark test using previously collected data. Not a prospective clinical trial. Not a real hospital workflow.
This post reviews what peer-reviewed research actually shows — how these tools work, where they excel, and where they fall short. (See Figure 1 for a visual overview of the entire AI-assisted genomic diagnosis workflow.)
Figure 1: AI-Assisted Genomic Diagnosis Workflow
What Is AI Genetic Diagnosis?
Quick Answer: AI genetic diagnosis uses machine learning to prioritize disease-causing variants from genome sequencing data (Changalidis et al., 2026).
Let us break that down. Our DNA is a string of 3 billion letters: A, T, G, and C. A variant is any place where your DNA differs from the reference genome. Most people have 3-5 million. A disease-causing mutation is the specific variant making you sick. Usually only one or two exist in your entire genome. AI scans all variants and ranks them by how likely each is to cause disease.
As Kim and colleagues (2024) explain, “previous variant prioritization tools mainly depend on in-silico prediction… which results in low sensitivity and difficulty in interpreting the prioritization result” (p. 2). AI offers a way forward. Figure 2 illustrates how each step of analysis progressively narrows the search space — from millions of total variants down to the single disease-causing mutation.
Figure 2: The Variant Funnel
A Patient Story: Meet Sarah
Sarah is eight years old. For five years, her parents have watched her struggle with seizures that medications cannot fully control. She has missed birthdays, school days, and playground games. Her parents are exhausted. They have seen neurologists, geneticists, and epileptologists. They have endured MRI scans, EEGs, and targeted gene panels. No diagnosis.
Her physician orders whole exome sequencing. The laboratory uses an AI prioritization tool. Out of approximately 22,000 initial variants, the AI flags 15 as high priority.
A genetic counselor reviews these candidates and identifies a mutation in KCNQ2. This gene causes a specific epilepsy syndrome. There is a targeted treatment.
Within months, Sarah’s seizures are better controlled. Her parents finally have an answer.
Note: This scenario is hypothetical — a composite based on published case reports, not a real individual. AI did not replace the genetic counselor. It provided a focused list. The human made the final call.
How Accurate Is AI Genetic Diagnosis?
Most published accuracy figures reflect retrospective benchmark performance, not clinical deployment accuracy. Understanding this hierarchy is essential. Table 1 below shows the current evidence levels available for AI genetic diagnosis tools — from retrospective benchmarks (widely available) to regulatory approval (none to date).
| Table 1: Evidence Hierarchy for AI Genetic Diagnosis | |
| Evidence Level | Current Status |
| Retrospective benchmark | Available |
| Cross-validation | Available |
| External cohort validation | Limited |
| Prospective clinical trial | Rare |
| Regulatory approval | None |
| Table 1: Most published accuracy figures reflect retrospective benchmark performance, not clinical accuracy. Source: Changalidis et al. (2026) | |
Table 2 summarizes benchmark performance data from peer-reviewed research for six leading AI tools.
| Table 2: Benchmark Performance from Peer-Reviewed Research | ||
| Tool | Performance | Source |
| V2P | >85% top-10 ranking | Stein et al., 2025 |
| 3ASC | 85.6% top 1 recall | Kim et al., 2024 |
| 3ASC | 94.4% top 3 recall | Kim et al., 2024 |
| Suggested Diagnosis | +12.5% diagnostic yield | Zucca et al., 2025 |
| MARRVEL-MCP | 94% benchmark pass rate* | Everton et al., 2026 |
| ClinVar-BERT | AUROC 0.927 for VUS | Li et al., 2026 |
| Table 2: Benchmark performance of selected genomic interpretation and clinical decision-support tools reported in peer-reviewed studies. | ||
Real AI Tools You Should Know About
- V2P (Nature Communications, 2025): Maps genetic variants to 23 Human Phenotype Ontology categories. “Our approach allows us to pinpoint the genetic changes that are most relevant to a patient’s condition” (Stein et al., 2025, p. 4).
- MARRVEL-MCP (AJHG, 2026): Allows plain-language queries like “Is this BRCA1 mutation linked to cancer?” Achieved 94% benchmark pass rate but “remains below the threshold required for autonomous clinical use” (Everton et al., 2026, p. 1208).
- 3ASC (Human Genomics, 2024): Explainable algorithm using 28 ACMG/AMP criteria. Shows which features drove each prediction — critical for clinical trust.
- ClinVar-BERT (Genome Medicine, 2026): Processes 2.3 million variant summaries. Prioritizes 7,644 variants for expert review, allowing panels to focus on 143 rather than thousands.
- Suggested Diagnosis (Human Genetics, 2025): Increased diagnostic yield by 12.5%, solving two previously undiagnosed cases.
The Generalization Gap
A 2025 systematic review identified major challenges: “integrating multimodal data… into unified and clinically robust pipelines, facing limitations in generalizability and practical implementation” (Changalidis et al., 2026, p. 5).
Documented limitations:
- Ancestry bias: Most models trained on European ancestry data; performance may drop for other populations (Ilić & Sarajlija, 2025)
- Phenotype quality: Models require structured HPO terms; clinics use unstructured notes (Stein et al., 2025)
- Novel syndromes: Models default to common diseases (Changalidis et al., 2026)
When AI Gets It Wrong
No AI system is perfect. What happens when the AI misses the mutation?
AI can fail for several reasons. These include incomplete phenotype data, underrepresentation of certain ancestries in training datasets, novel disease mechanisms not captured in training data, or technical sequencing artifacts.
Consequences vary. In the best cases, the correct variant remains in the candidate list despite a lower ranking. In the worst cases, it is excluded entirely, delaying diagnosis, increasing costs, and prolonging the diagnostic odyssey.
Mitigations exist. Laboratories do not rely on AI outputs alone. All variants are reviewed by trained experts using clinical evidence, family history, and established interpretation guidelines (Changalidis et al., 2026). Multiple AI tools can be run in parallel. Human experts also regularly audit AI outputs.
This is why autonomous AI diagnosis does not exist today and why human oversight remains essential.
Privacy, Bias, and Explainability
- Privacy: Genetic data cannot be changed like a password. It reveals information about blood relatives. Before using any AI tool, ask: Where is my data stored? Who has access? Can I withdraw consent?
- Bias: Models trained primarily on European ancestry may perform worse for African, Asian, or Latino patients. No AI genetic diagnosis tool has been formally audited for bias across all population groups.
- Explainability: Many deep learning models are “black boxes.” Some tools (like 3ASC) use explainable AI techniques. Always ask: Can your AI explain why it prioritized a specific variant?
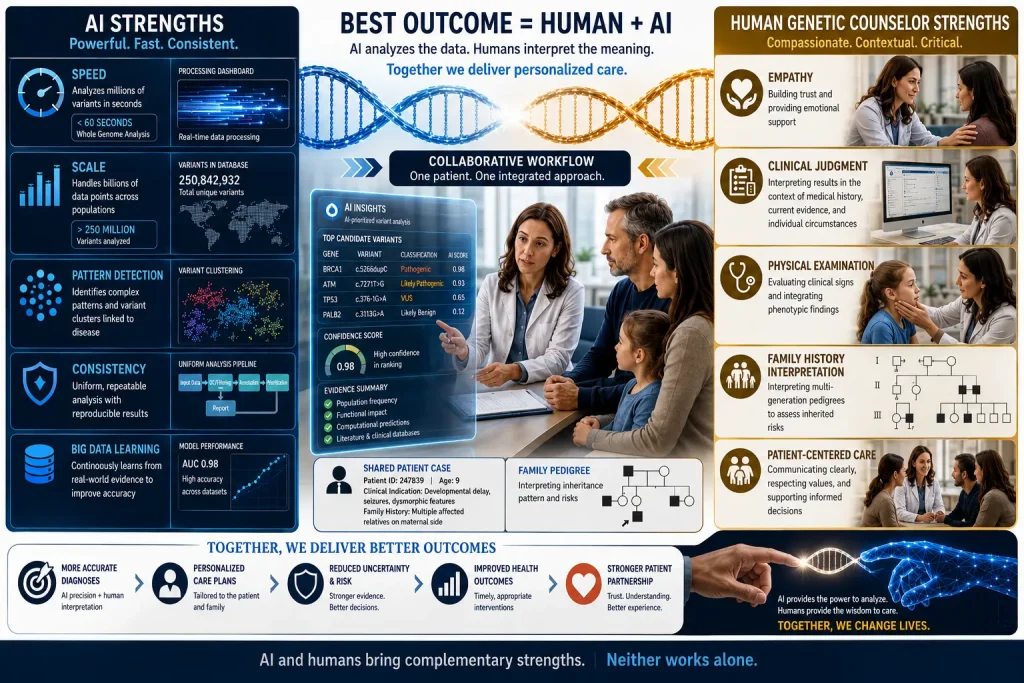
What Humans Do That AI Cannot
Table 3 lists specific clinical tasks that remain exclusively in the human domain — tasks AI cannot perform regardless of future advances.
| Table 3: Human Strengths AI Cannot Replicate | |
| Human Task | Why AI Cannot Do It |
| Taking a family history | Requires conversation and follow-up questions |
| Performing a physical exam | Requires observation and touch |
| Integrating multisystem findings | AI sees variants; humans see the whole patient |
| Explaining results to families | Requires empathy and translation |
| Making the final diagnosis | AI produces probabilities; humans make deterministic decisions |
| Detecting AI errors | AI cannot self-criticize |
The optimal model is partnership. AI handles speed and scale. Humans provide context, empathy, and judgment. (See Figure 3 for a visual comparison of AI and human strengths, and why the best outcome comes from combining both.)
Figure 3: Why AI Cannot Replace Genetic Counselors
The Future of AI Genetic Diagnosis
Based on a systematic review of 195 studies (Changalidis et al., 2026):
| Direction | Source |
| Personalized medicine matching treatments to profiles | Stein et al., 2025 |
| Multimodal integration (genomics + imaging + clinical) | Changalidis et al., 2026 |
| Accessible, locally installable models | Everton et al., 2026 |
| VUS reclassification | Li et al., 2026 |
| Explainable AI for clinical trust | Kim et al., 2024 |
| Bias mitigation and diverse training data | Ilić & Sarajlija, 2025 |
The field is moving from proof-of-concept to clinical integration. The next five years will determine whether these tools achieve widespread adoption.
Key Takeaways
- AI acts like a metal detector — narrowing millions of variants to a handful of candidates
- Benchmark performance: V2P >85% top-10; 3ASC 85.6% top 1 recall; MARRVEL-MCP 94% pass rate
- These figures reflect retrospective benchmarks, not clinical accuracy
- No AI system has regulatory authorization for autonomous diagnosis
- Major limitations: ancestry bias, privacy, lack of explainability
- AI is decision support — not replacement for genetic counselors
- The optimal model is partnership: AI handles pattern recognition; humans make final diagnoses
- Always ask: How was this validated? For whom does it work? Who has access to my data?
Conclusion: The Metal Detector Finds Metal. You Dig.
Think of it like that metal detector on the beach. The detector finds the metal. You dig. You find the earring. Neither works alone.
AI genetic diagnosis is transforming variant prioritization. Peer-reviewed research validates strong benchmark performance. But significant limitations remain: generalizability gaps, lack of prospective validation, privacy concerns, algorithmic bias, and no regulatory approval for autonomous use.
The optimal path forward is partnership. As Everton and colleagues (2026) conclude, the appropriate role for AI is “decision-support that accelerates expert workflows rather than replacing judgment”.
If you work in healthcare, ask your genetics team: “What AI tools are you using? How have they been validated? For whom do they work? How do you protect patient data?” The questions themselves drive progress.
About the Author
Dr. Niamat Khan, PhD (Germany) is a geneticist with 16+ years of experience in rare disorders and cancer genomics, researching AI applications in genetic diagnosis at Kohat University of Science and Technology.
References
- Changalidis, A., Barbitoff, Y., Nasykhova, Y., & Glotov, A. (2026). A systematic review on the generative AI applications in human medical genetics. Frontiers in Genetics, 16, 1694070. https://doi.org/10.3389/fgene.2025.1694070 (Open Access)
- Everton, Z., Botas, J., Kim, S. Y., Yao, L., Liu, Z., & Jeong, H. H. (2026). MARRVEL-MCP: An agentic interface for Mendelian disease discovery via tool-augmented context engineering. American Journal of Human Genetics, 113(6), 1194-1213. https://doi.org/10.1016/j.ajhg.2026.04.012 (Requires Institutional Access)
- Ilić, N., & Sarajlija, A. (2025). Artificial intelligence in the diagnosis of pediatric rare diseases: From real-world data toward a personalized medicine approach. Journal of Personalized Medicine, 15(9), 407. https://doi.org/10.3390/jpm15090407 (Open Access)
- Kim, H. H., Kim, D. W., Woo, J., & Lee, K. (2024). Explicable prioritization of genetic variants by integration of rule-based and machine learning algorithms for diagnosis of rare Mendelian disorders. Human Genomics, 18(1), 28. https://doi.org/10.1186/s40246-024-00595-8 (Open Access)
- Li, W., Li, X., Lavallee, E., Saparov, A., Zitnik, M., & Cassa, C. (2026). From text to translation: Using language models to prioritize variants for clinical review. Genome Medicine. Advance online publication. https://doi.org/10.1186/s13073-026-01661-7 (Open Access)
- Stein, D., Kars, M. E., Milisavljevic, B., et al. (2025). Expanding the utility of variant effect predictions with phenotype-specific models. Nature Communications, 16, 11113. https://doi.org/10.1038/s41467-025-66607-w (Open Access)
- Zucca, S., Nicora, G., De Paoli, F., Carta, M. G., Bellazzi, R., Magni, P., Rizzo, E., & Limongelli, I. (2025). An AI-based approach driven by genotypes and phenotypes to uplift the diagnostic yield of genetic diseases. Human Genetics, 144(2-3), 159-171. https://doi.org/10.1007/s00439-023-02638-x (Open Access)